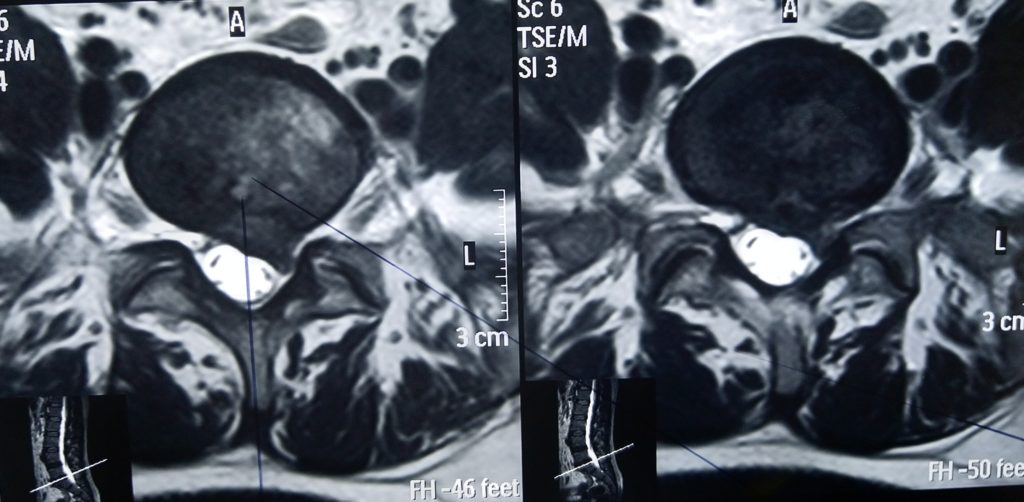
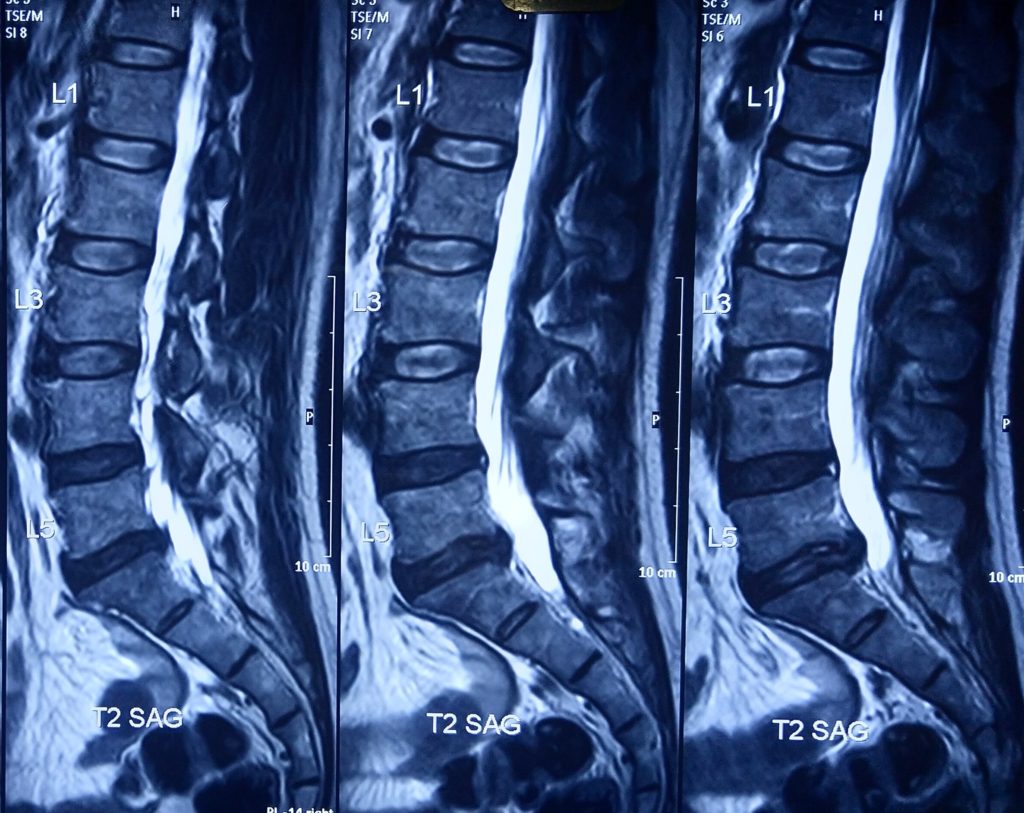
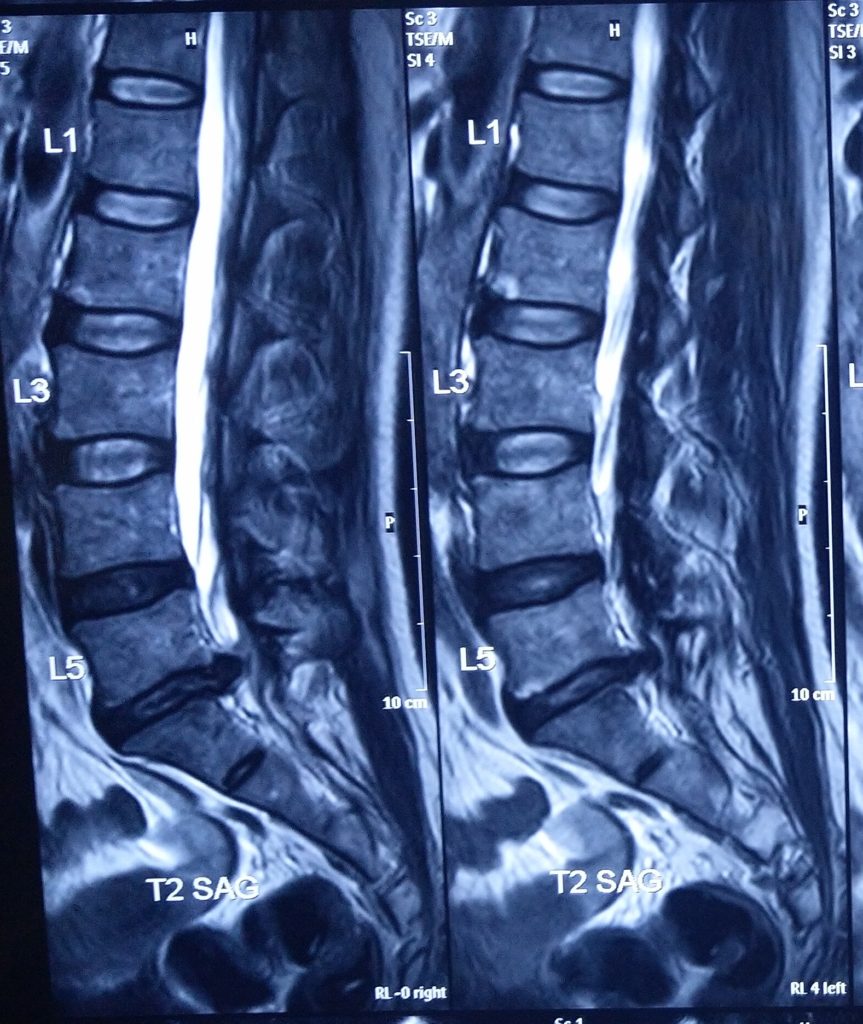
47 years male presented with left sciatic list, not able to stand for a while & literally he was crying with pain .
Clinical Examinaton: –
Left Ankle Jerk was absent, SLR was left side 100 & on right side contralateral positive on 300.
Diagnosis: –
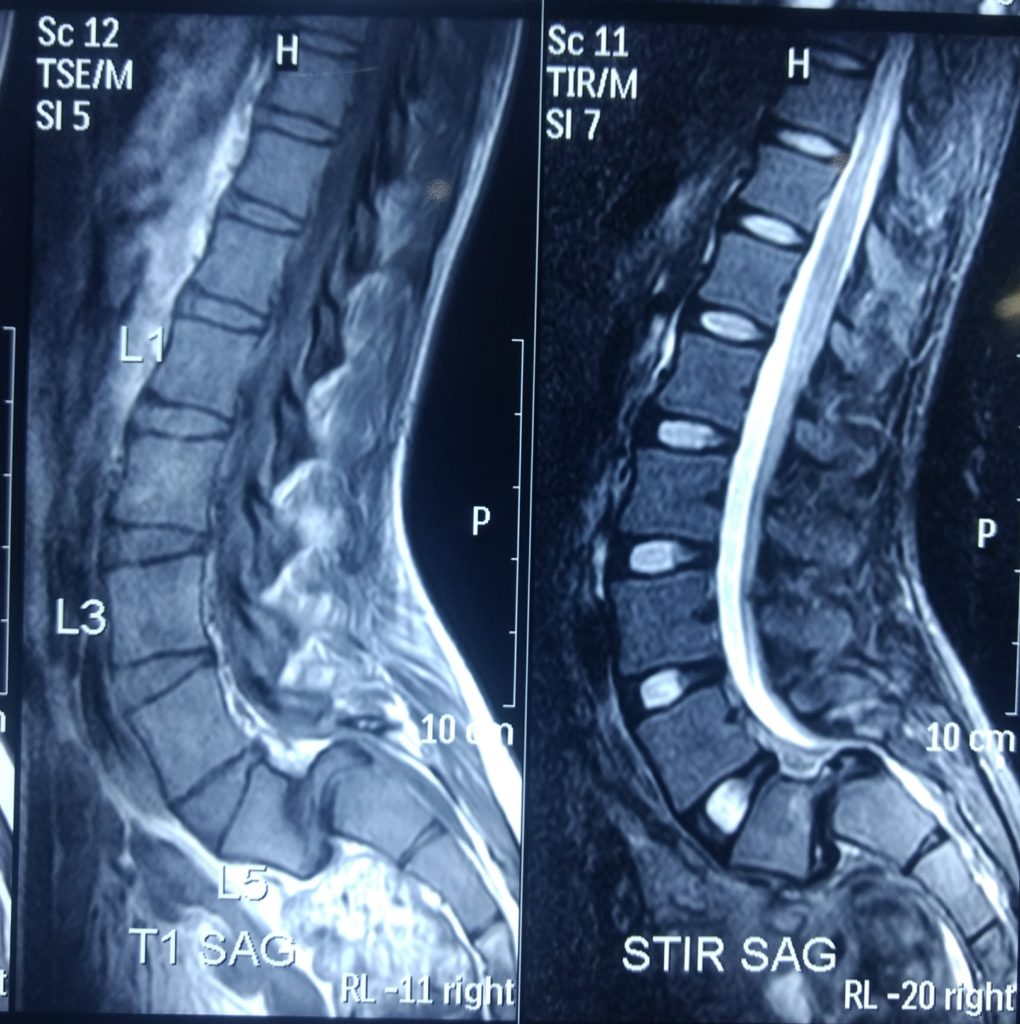
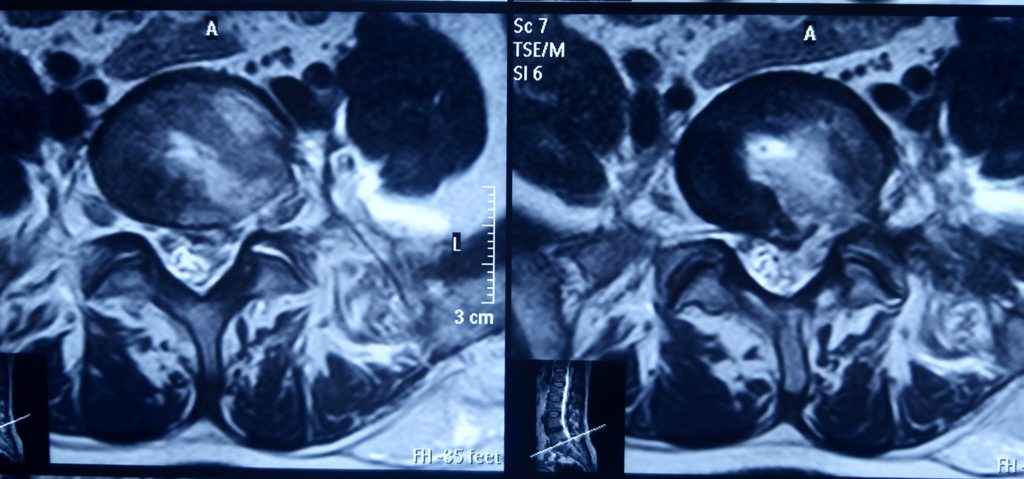
After MRI left centro paracentral upmigrated large disc at L5-S1 with very high iliac crest.
Surgery: –
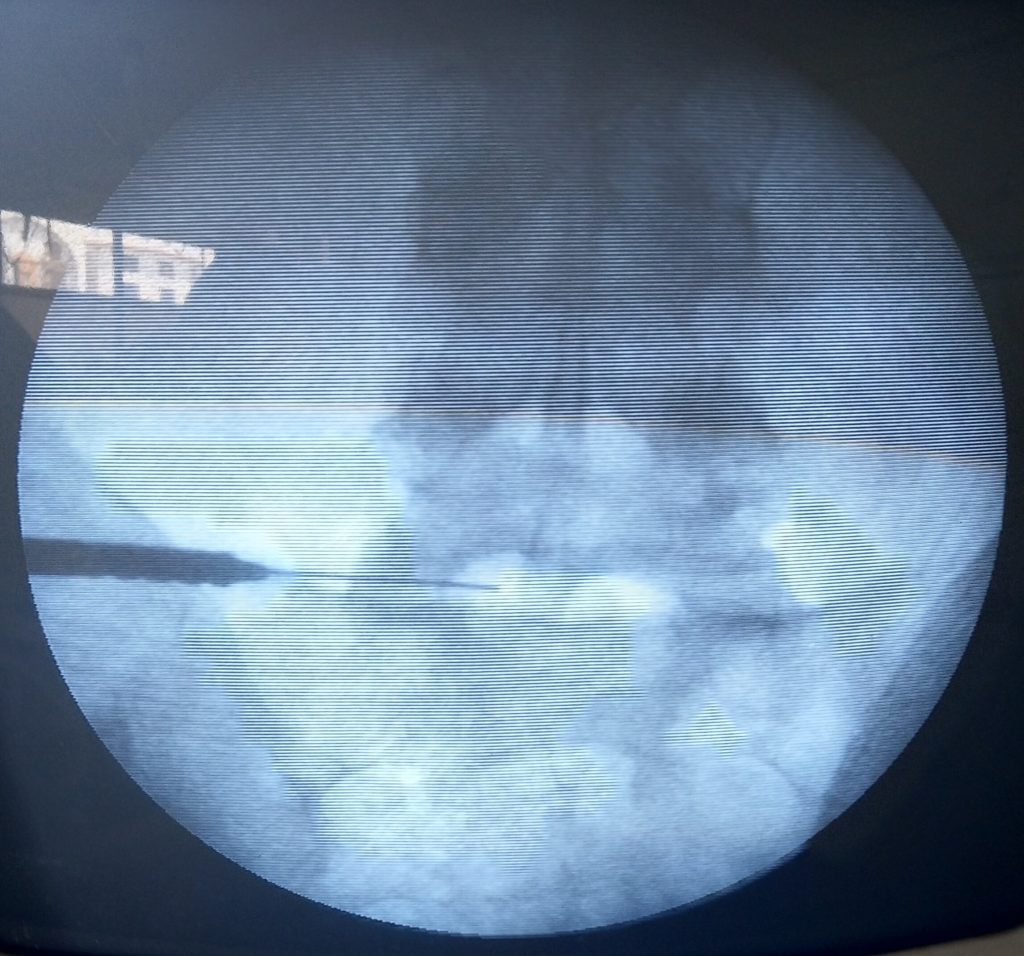
Transiliac Transforaminal Endoscopic Disccectomy Under Local Anaesthesia.
Results: –
Patient got immediate relief in radiating pain started to walk just after surgery. He discharged on next morning of surgery & he joined his job from 3rd day of surgery. Now he is doing all types of his work like weight lifting, running, squatting..etc.
Patient Speak: –
Highly satisfied.




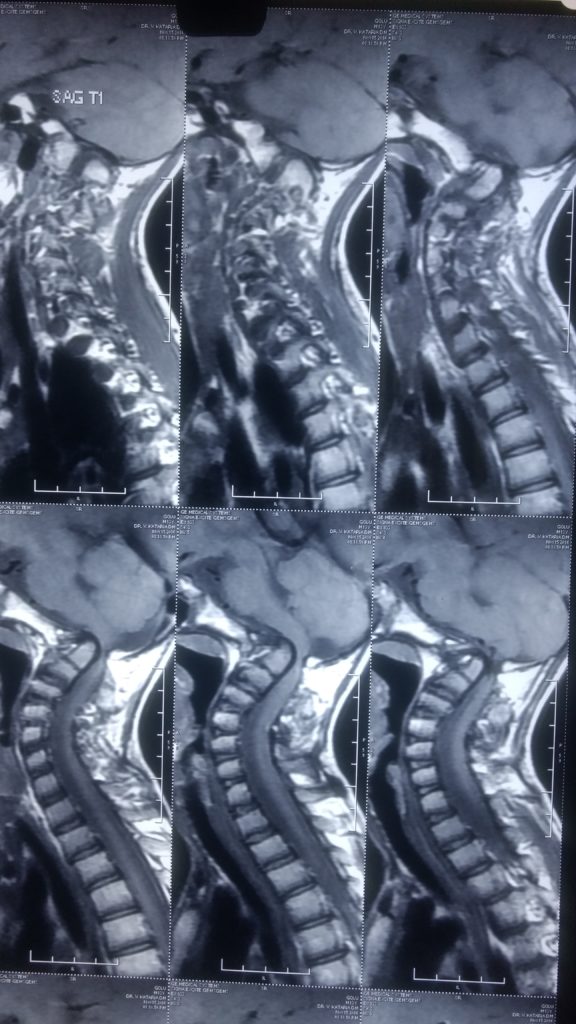
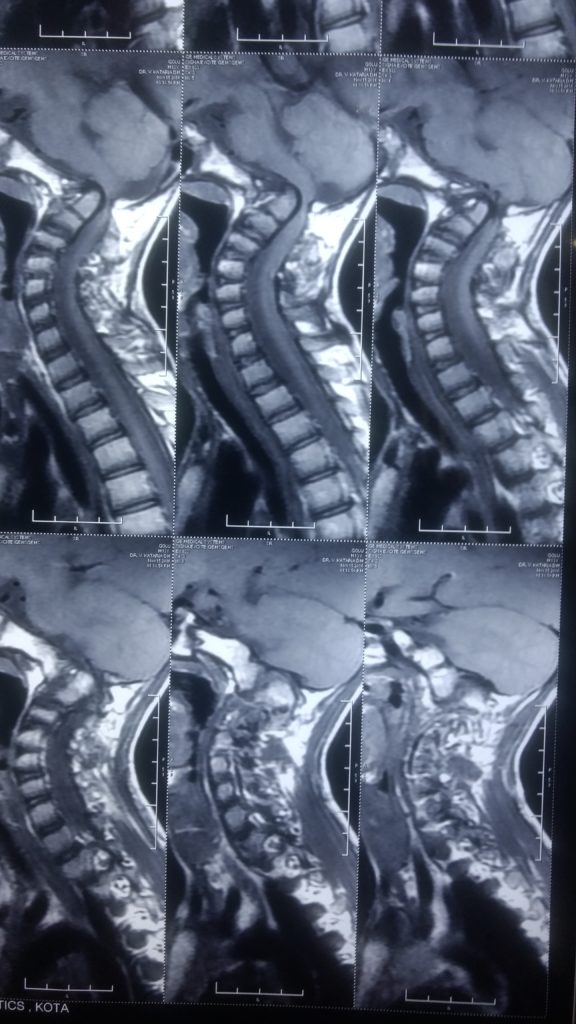
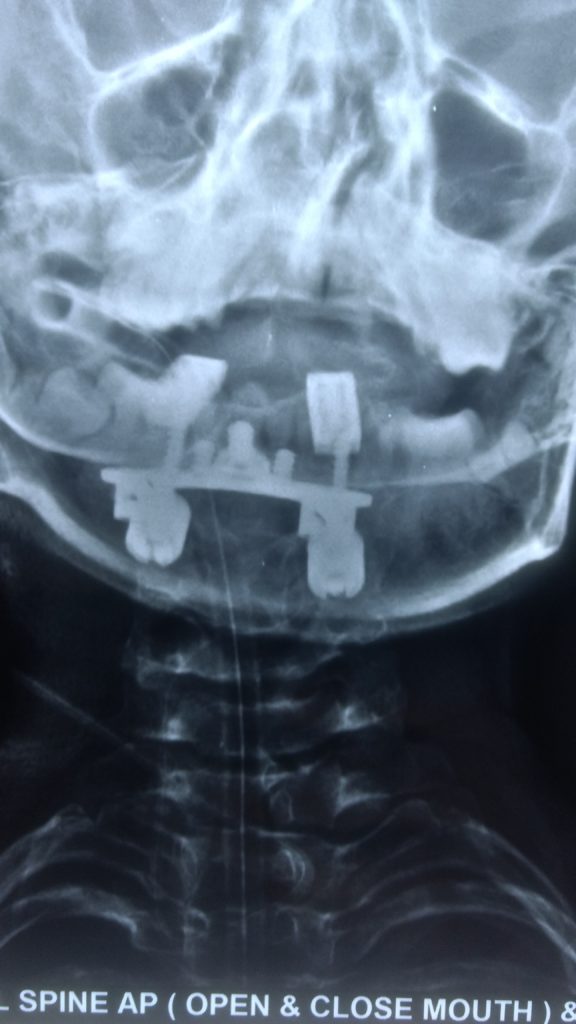
15 year old child presented with history of Fell down from bicycle & went to home by self uneventfully. After one month he felt some weakness in both lower limbs & got bed ridden within 4 months of incidence, not able to walk or stand due to complete weakness of lower limbs then weakness started in both upper limb & difficulty in breathing.
Clinical Examination: –
All DTR Brisk, Spasticity in all 4 limbs, Ankle & Patellar clonus +nt, Plantar reflexes: Extensor, chest expansion 2.5 cm.
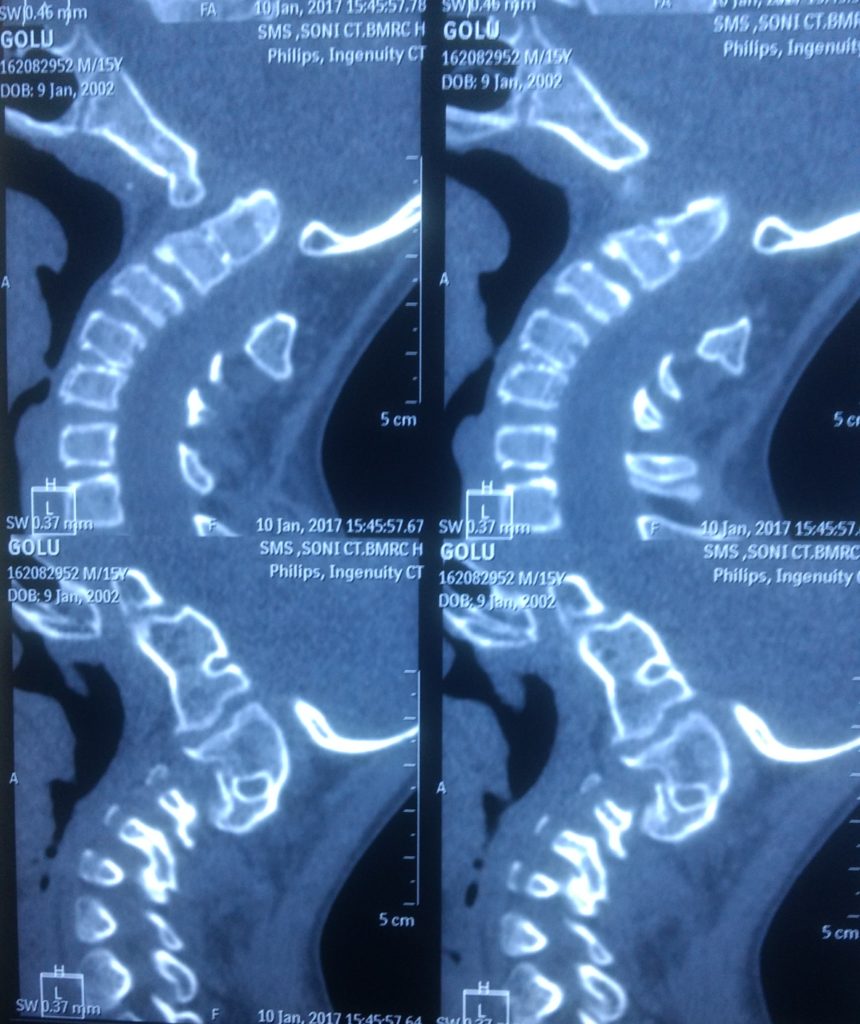
Diagnosis: –
Non reducible Atlanto Axial Dislocation with Basillar Invasion (AAD with BI).
Challenges: –
We put him on skeletal traction, but AAD not reduced so it was challenge to reduce, & always these type of patient has high risk for surgery, & this patient has already poor vital capacity so we operated him after written consent of DOT.
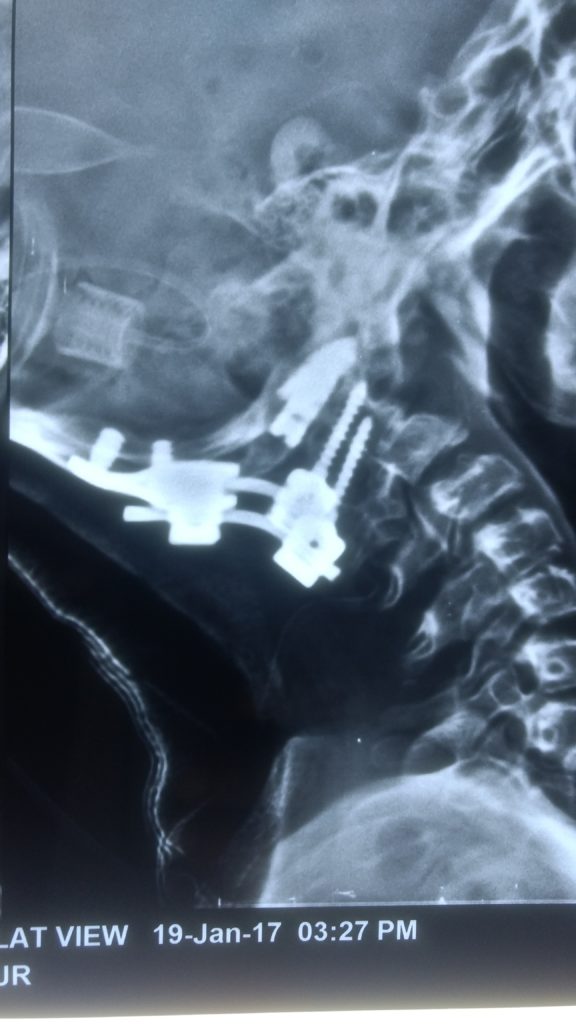
Surgery: –
Laminectomy, Foramen magnum decompression, OC2C3 fixation, & put C1C2 cage both side & fusion with bone Graft.
Results: –
Patient got neurological improvement one month after surgery, now he is living his normal life.
Patient Speak: –
Highly satisfied.


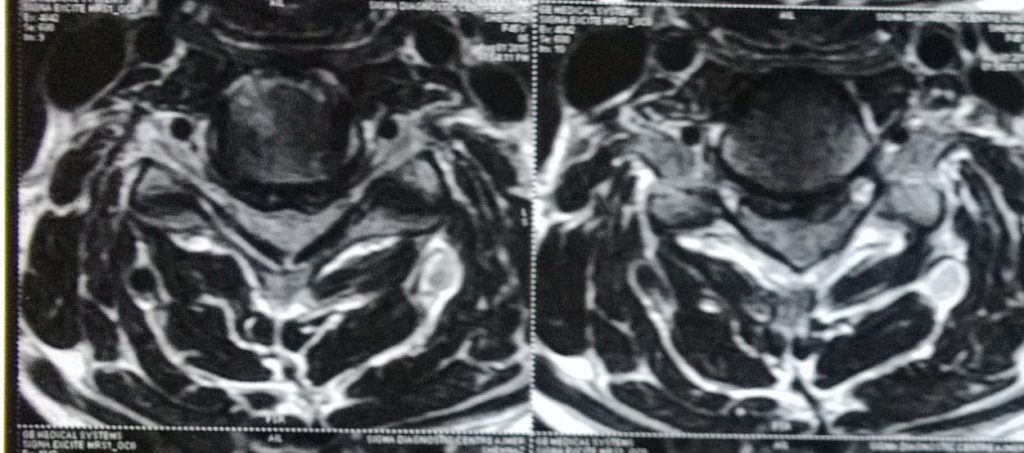
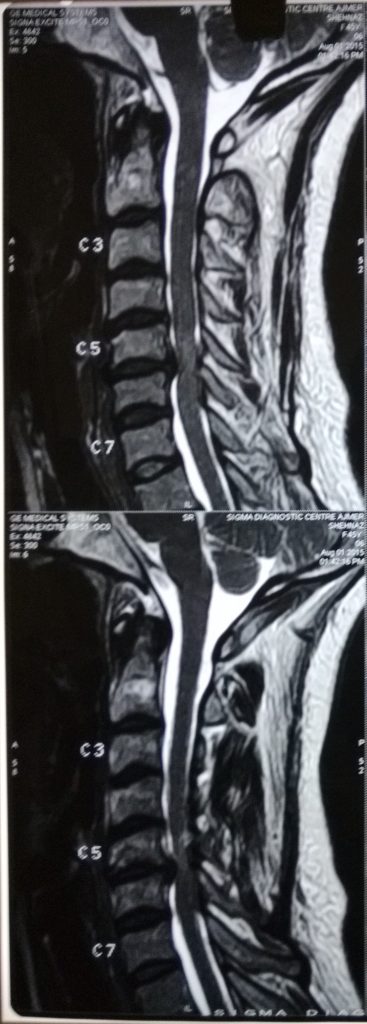
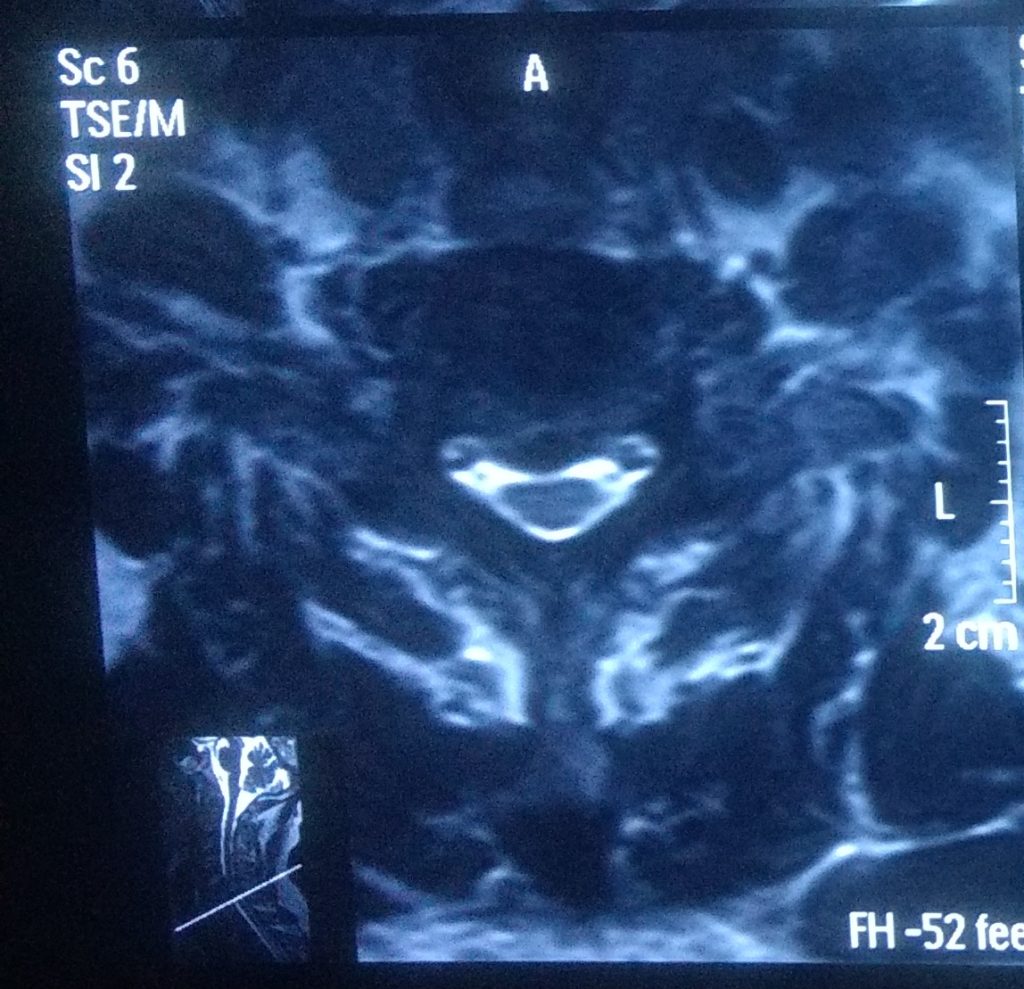
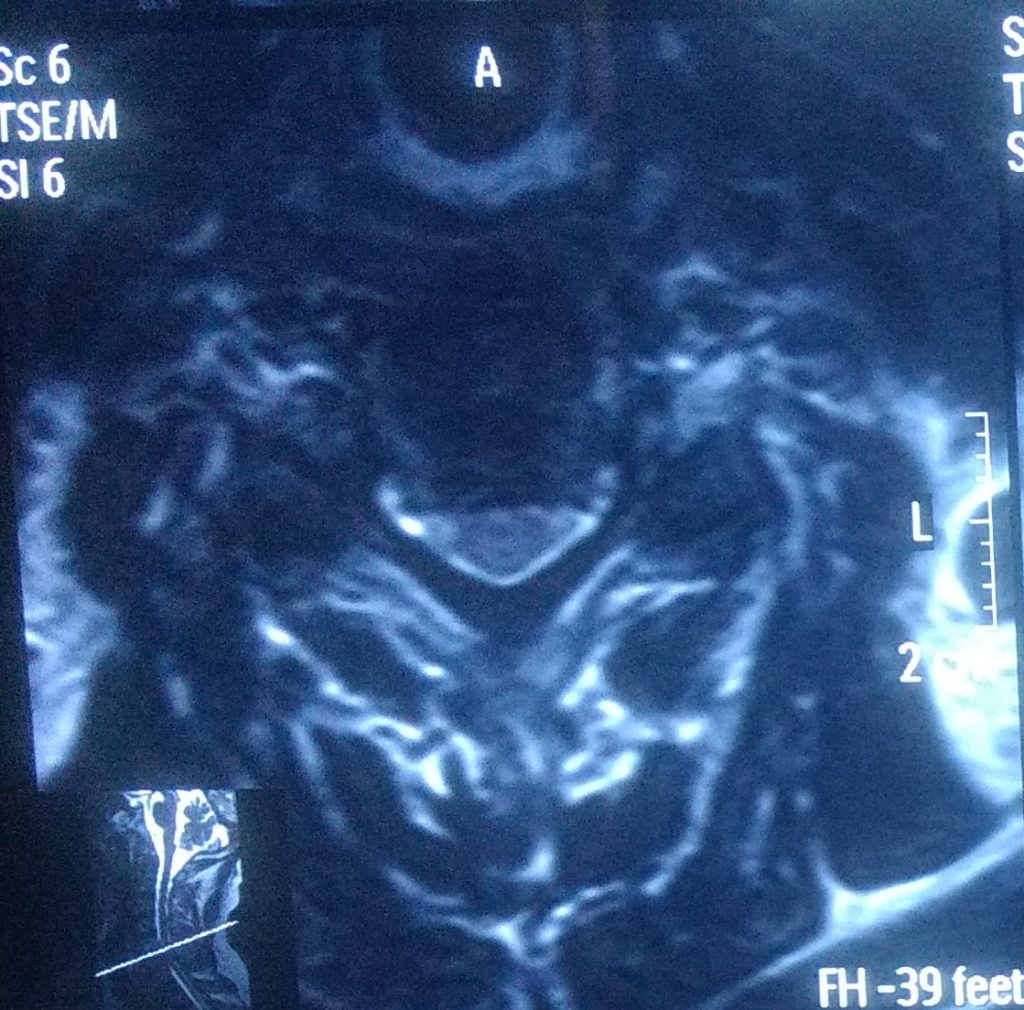
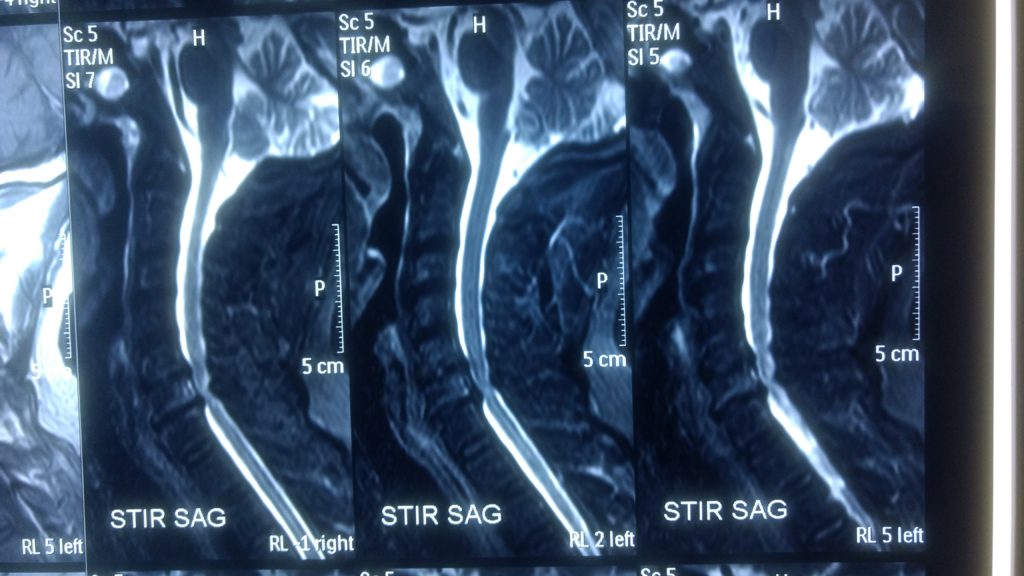
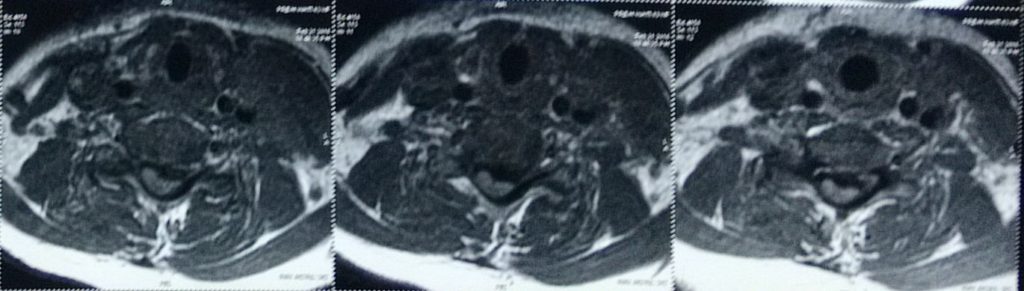
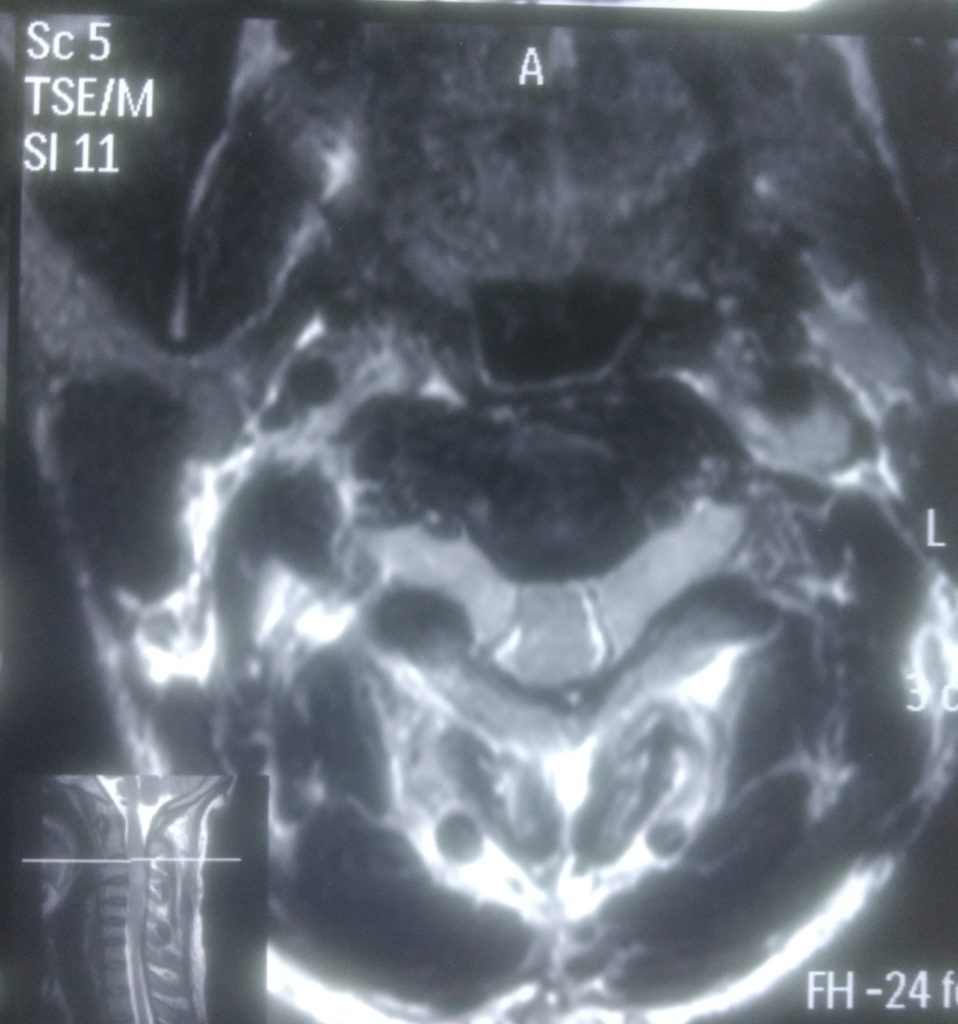
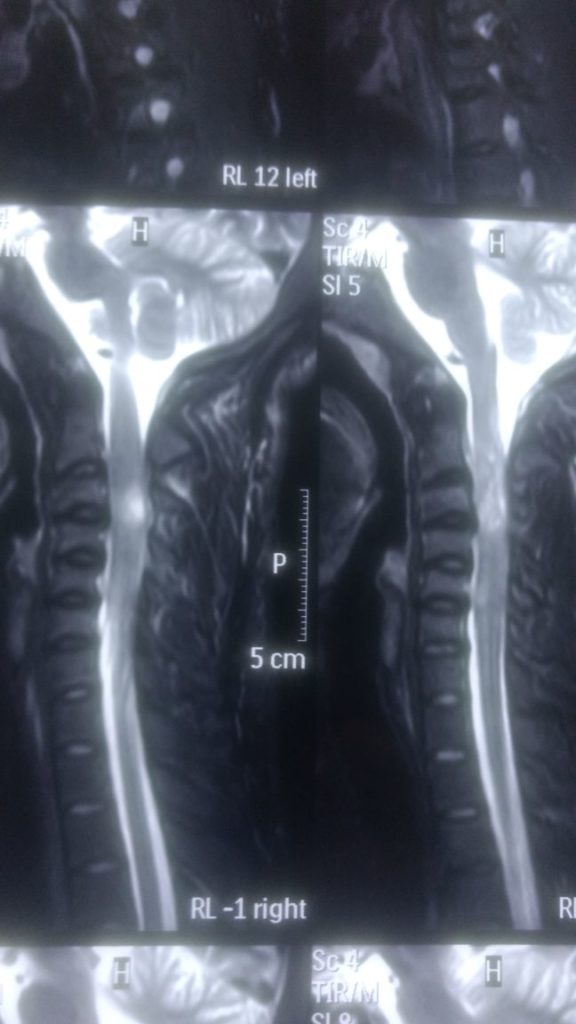
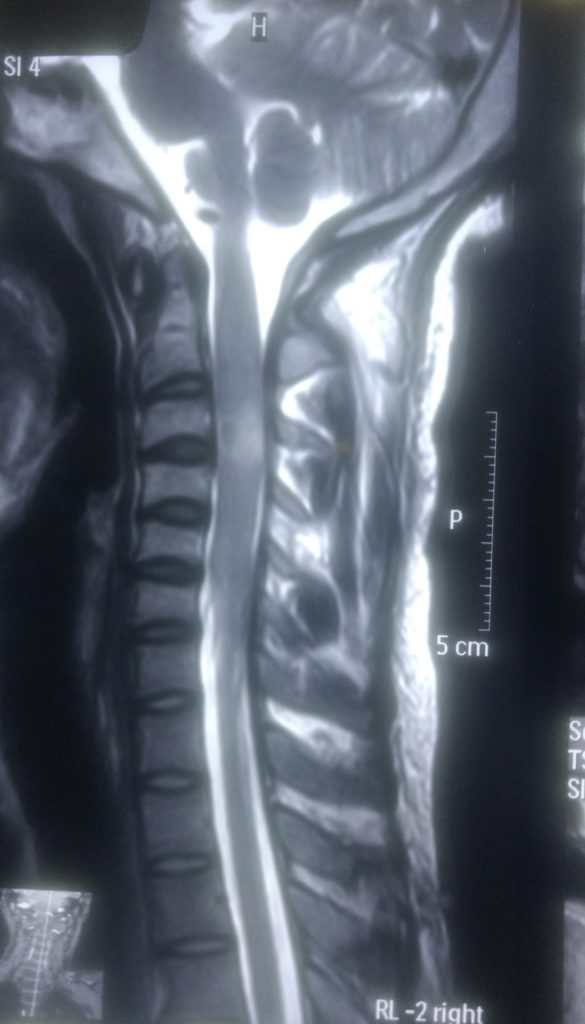
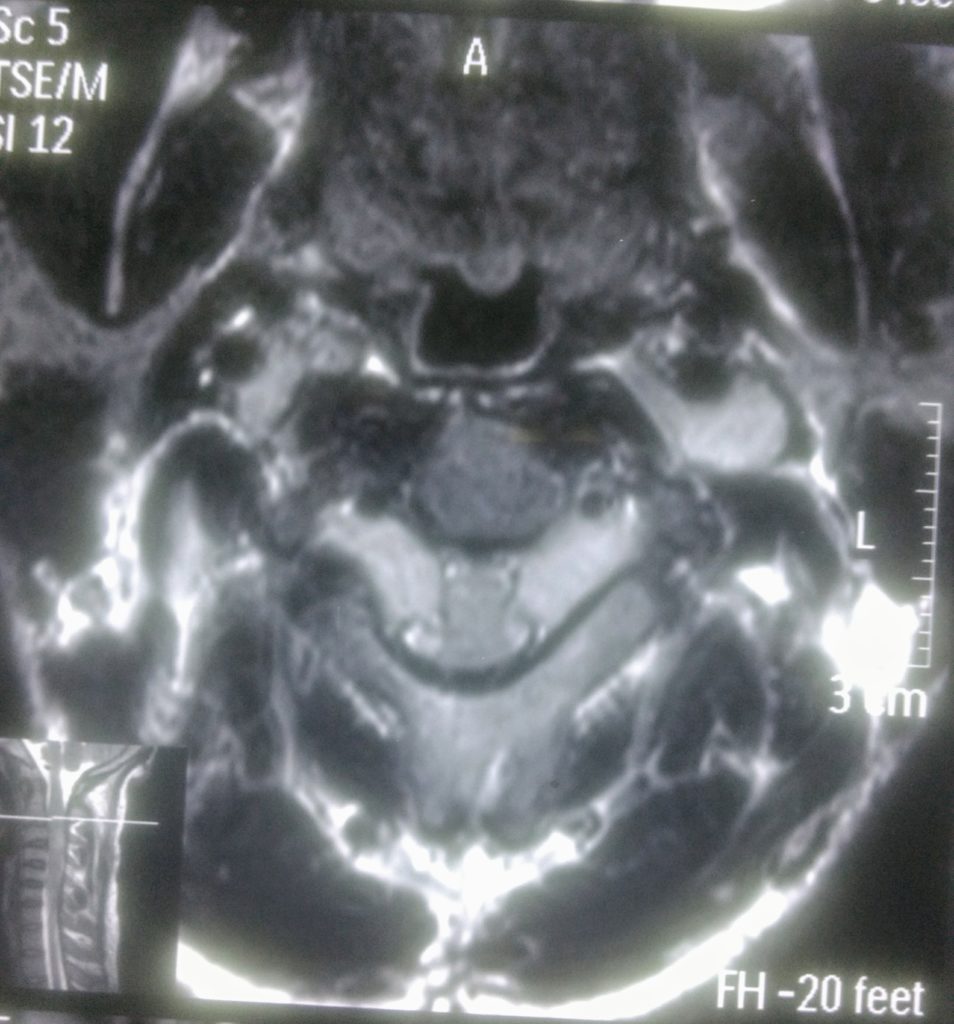
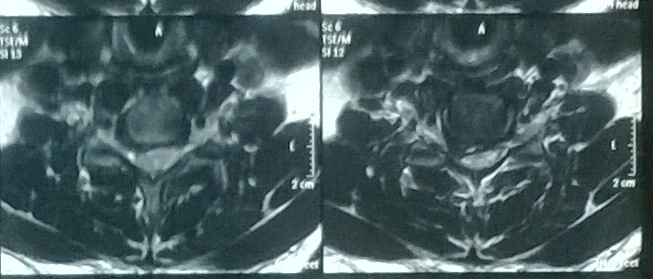
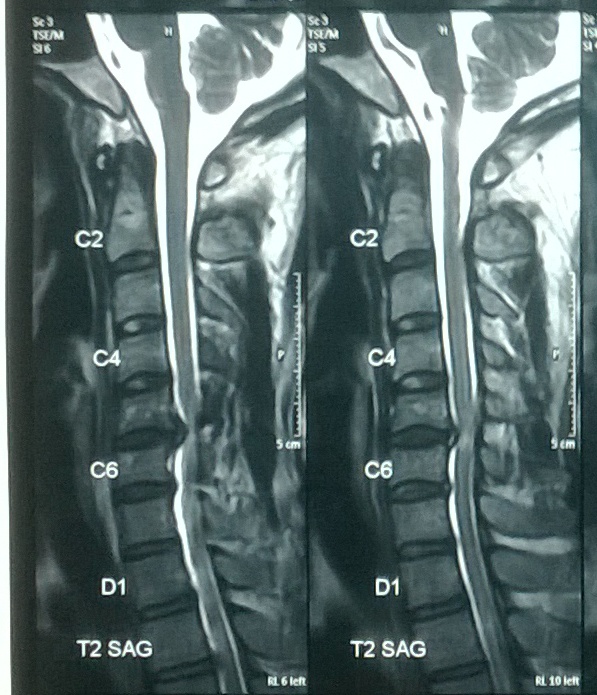
53 year old female has complains of neck pain from 12 years radiated to both upper limbs from 08 years gradually she felt weakness in both upper limbs.
Clinical examination: –
Motor (Power) weakness in both hands & at elbows, diminished sensations over forearm.
Diagnosis: –
After MRI she diagnosed large PIVD (Slip disc) at C5-C6 level, compressing spinal cord.
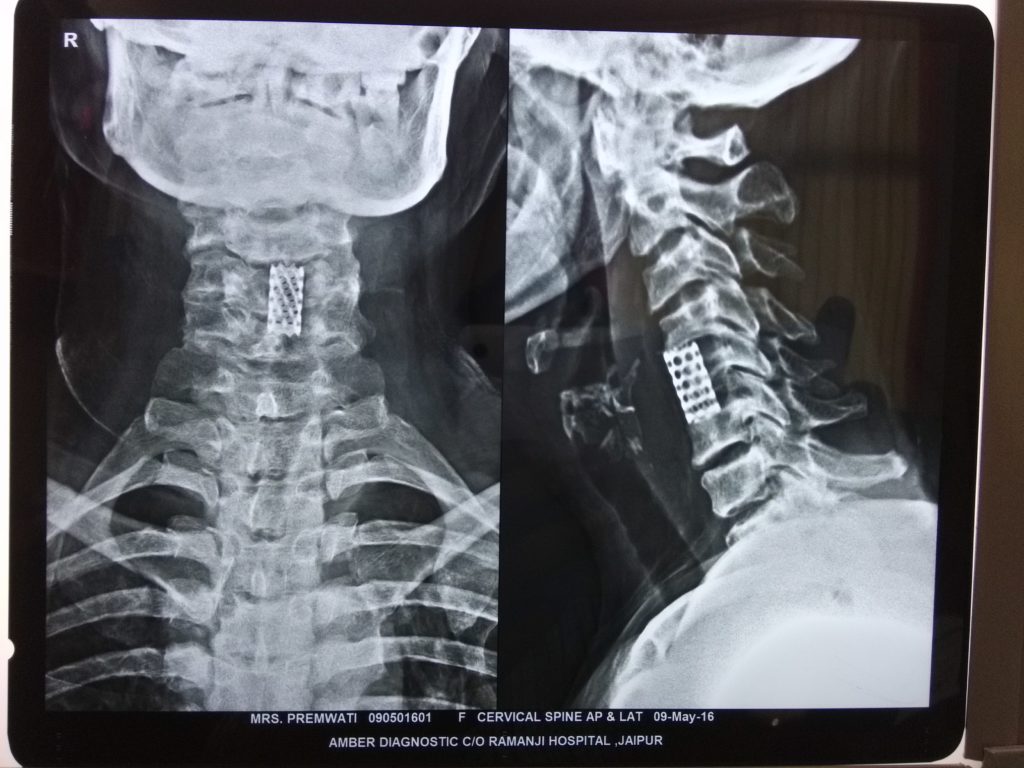
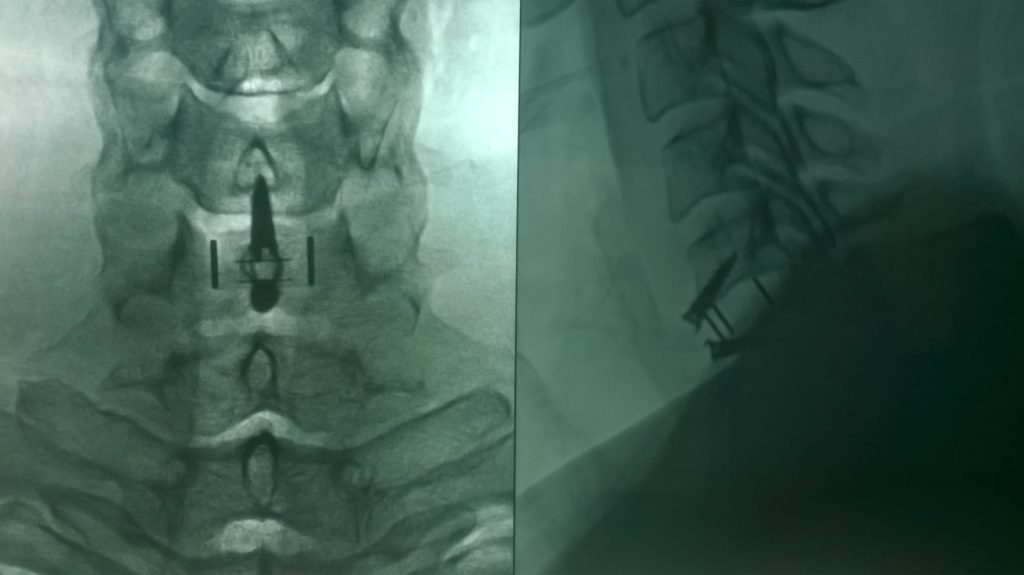
Surgery: –
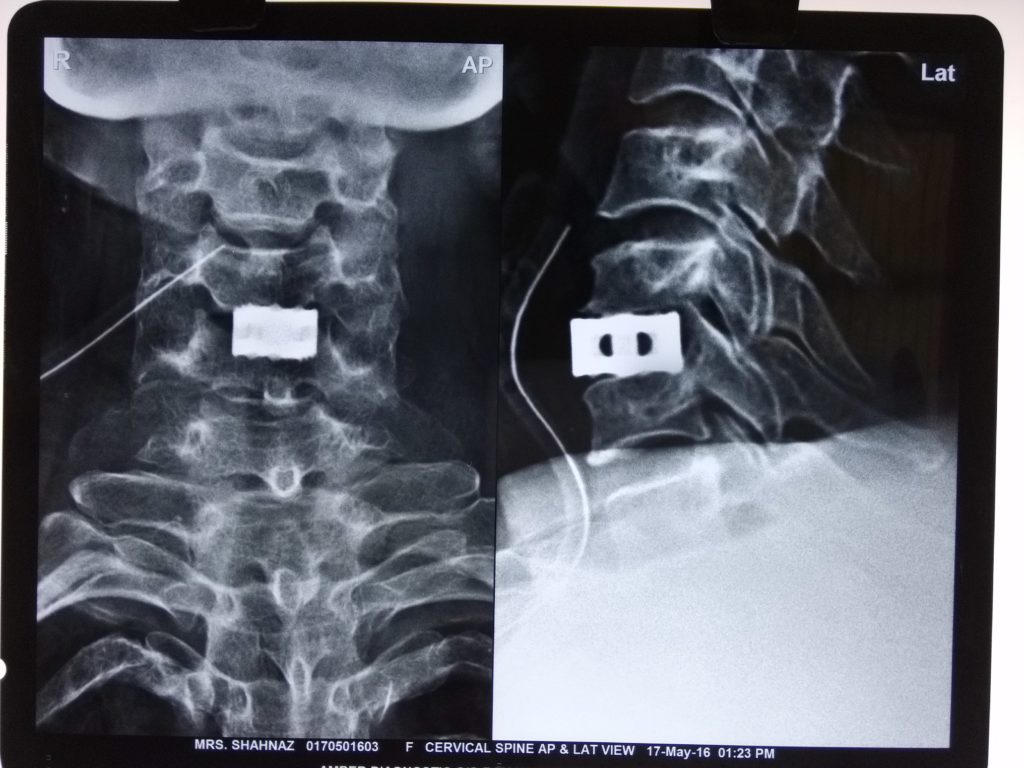
ACDF (Anterior cervical discectomy, fixation & fusion with bone graft) with Stand Alone Cage.
Results: –
She got relief in radiating pain immediately after surgery & gained motor power within a year after surgery.
Patient Speak: –
Highly satisfied.
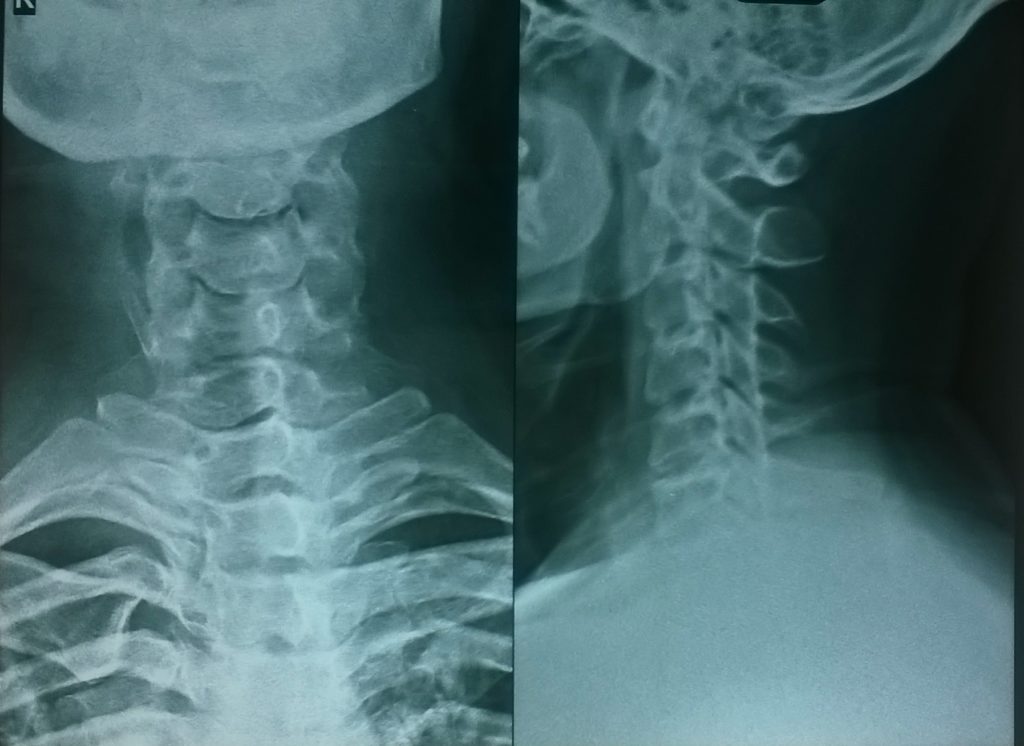
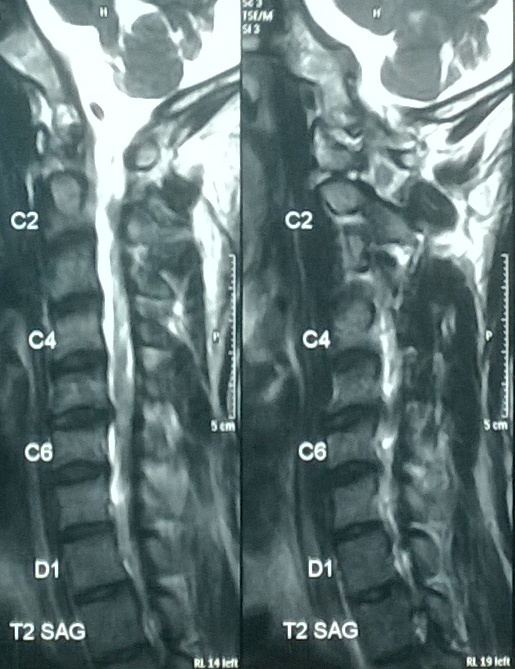
63 years male has cervical pain from 15 years , got radiating pain then weakness to both upper limbs, gradually felt gait imbalance, at time of presentation he was not able to stand or walk straight not more than 2-3 minutes.
Clinical Examination: –
He had weakness in both upper limb, Biceps/ triceps & supinator reflexes weak, spastisity , clonus in both lower limbs, KJ, AJ exaggerated, plantar reflex was extensor.
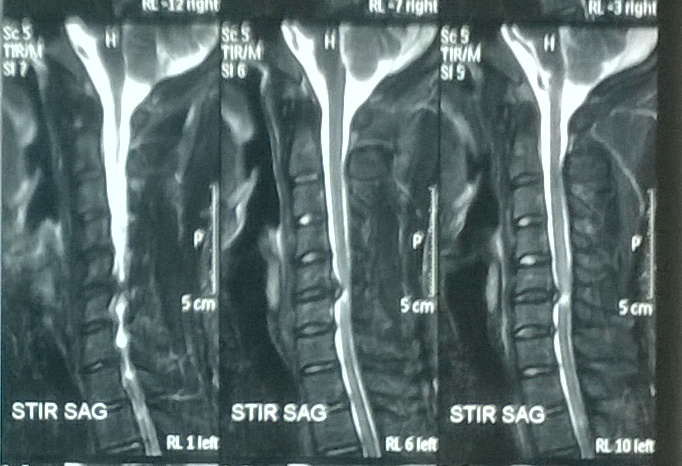
Diagnosis: –
Cervical Myelopathy with 2 level PIVD (C5-C6, C6-C7) & Ossification of PLL.
Surgery: –
He operated with Corpectomy , Diskectomy ,Fixation & Fusion with Stand Alone Cage.
Results: –
Radiating pain relief completely just after surgery , spasticity & motor weakness improved within 16 months.
Patient Speak: –
Highly satisfied.



50 year male presented with cervical pain from 10 years gradually pain aggravated & felt weakness to grip the articles, then felt gait imbalance.
Clinical Examination: –
Biceps: Left side absent, Triceps: Both sides Normal, hand grips weak (L>R), both sides AJ & KJ Eaggerated, Plantar Both sides Mute, Spasticity in both lower limbs present.
Diagnosis: –
Cervical Myelopathy at C5-C6 level due to large PIVD (Slip Disc) at C5-C6 level.
Surgery: –
ACDF with Stand Alone Cage.
Results: –
Post operatively hand grip & gait Imbalance improved.
Patient Speak: –
Highly satisfied.
50 years old male had History of fall from height and got Quadriparesis (complete weakness of both lower limbs & partial weakness of both upper limb) due to injury at neck.
Presentation In Hospital: –
He admitted in our hospital after 5 days of trauma
Clinical examination: –
He had 2/5 motor power on both upper limb while 0/5 power in both lower limbs & respiration was not good.
Diagnosis: –
C6-C7 fracture & dislocation with cord oedema & compression.
Management & Surgery: –
He managed in ICU & put him on skull traction & operated after 3 days with Reduction Fixation with plate & fusion with autograft.
Results: –
Post operatively pt improved in motor power now after 2 years he is able to stand & walk with support.
Patient Speak: –
Highly satisfied.
54 years male got Quadriparesis (complete weakness of both lower limbs & partial weakness of both upper limb) due to injury at neck. ( C6-C7 fracture & dislocation with cord oedema & compression) after history of fall from height.
Presentation In Hospital: –
Presented in our hospital after 3 days of trauma.
Clinical examination: –
He had 2/5 motor power on both upper limb while 0/5 power in both lower limbs.
Management & Surgery: –
He managed in ICU & put him on skull traction & achieved reduction, shifted in OT on traction on 4th day of admission Open Reduction fixation with plate & Fusion with Autograft.
Results: –
Post operatively no improvement in motor power & discharged after complete stable, but after suture removal he didn’t come in follow up.
Patient Speak: –
Highly satisfied.
61 years female has cervical pain from 08 years , after lifting heavy weight, got radiating pain then weakness to both upper limb (left>right) , gradually felt gait imbalance. At time of presentation she was not able to stand or walk straight not more than 8-10 minutes.
Clinical Examination: –
She had weakness in both upper limb (left>Right), Bicepts/ triceps & supinator reflexes weak, KJ, AJ exaggerated, plantar reflex was Mute.
Diagnosis: –
Cervical Myelopathy with 2 level PIVD (C4-C5, C5-C6) & Ossification of PLL.
Surgery: –
Corpectomy & diskectomy fixation & fusion with Stand Alone Cage.
Results: –
Radiating pain relief completely just after surgery, motor weakness improved within a year.
Patient Speak: –
Highly satisfied.

23 year boy had history of tingling, radiating sensations in both upper limbs from 2 years, gradually he felt stiffness in all limbs from 10 months & not able to stand, or walk for a while due to spaticity & gait imbalance at time of presentation.
Clinical Examination: –
All DTR Brisk, Spasticity present in all 4 limbs, Plantar reflexes B/L Extensor, Ankle Clonus Present, Shaking body on standing & hard to move one or two step even with support.
Diagnosis: –
He was a diagnosed case of neurofibroma, after MRI cervical spine he diagnosed neurofibroma C2-C3 level with changes in spinal cord (myelopathy).
Surgery: –
He operated from posterior with Laminectomy & excised tumor.
Complication: –
He had CSF leak for up to 20 days for which he reoperated from posterior & put duraseal at dural tear. Later on wound healed.
Results: –
He got relief in spasticity immediately & started to walk without support from 3rd day of surgery.
Patient Speak: –
Highly satisfied.

38 year male doctor had neck pain from 5 years then severe radicular pain in Rt upper limb, then felt weakness in griping of pen ( didn’t able to his signature).
Clinical Examination: –
Motor power weak, diminished sensations over forearm, Biceps reflex Rt side absent & left side diminished.
Diagnosis: –
Large sequestrated disc at C5-C6 compressing Rt lateral recess.
Surgery: –
Operated with ACDF ( Cervical Diskectomy & fixation with fusion).
Results: –
Post operatively got immediate relief in radiating pain, hand grip improved within 2 months of surgery, now he is able to do his all activities.
Patient Speak: –
Highly satisfied.
46 years male had difficulty in walking & didn’t able to look forward in up right posture, Kyphotic Deformity at Back (“KUBAD” ).
Clinical Examination & Investigation : –
Globular Kyphotic Deformity, Kyphotic angle around 870 , No neurological deficit, Forward gage 0, All tests for Ankylosing Spondilitis (AS) +ve, HLA B 27 Positive.
Diagnosis: –
Globular Kyphosis (angle 870) Due to AS.
Challenges: –
Hard Intubation, & giving prone position in such rigid deformity.
Surgery: –
He operated with two level Pedical Subtraction Osteotomy (PSO) & fixation with multi level Pedicle screws & fusion with bone graft.
Results: –
He started to walk from next day of surgery & got very good correction in deformity.
Patient Speak: –
Highly satisfied.
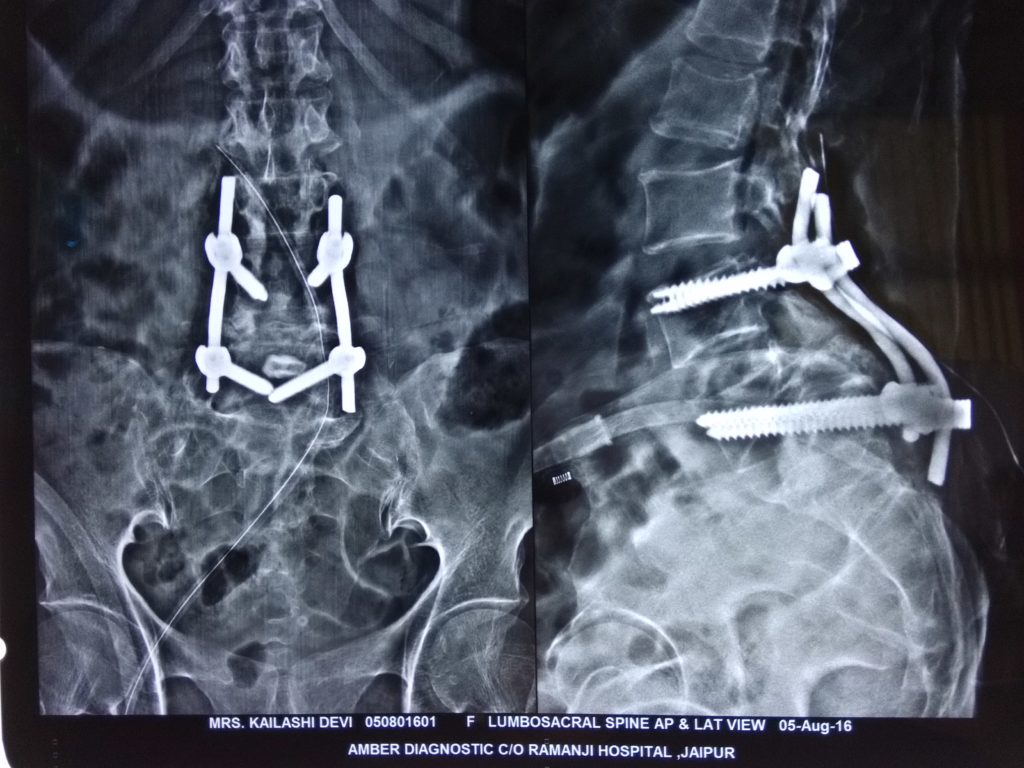
53 year old lady had LBA from 12 years, radiating pain in both lower limbs from 08 years, difficulty in walking from 05 years gradually she started to walk with support then she felt that she didn’t able to walk straight up right, always stand or walk with one side tilting trunk, when she presented our clinic was not able to walk or stand not more than 10 minutes ven with support.
Clinical Examination & Investigation: –
Ankle jerk Both side absent, Hypoesthesia in S1 Dermatome.
Diagnosis: –
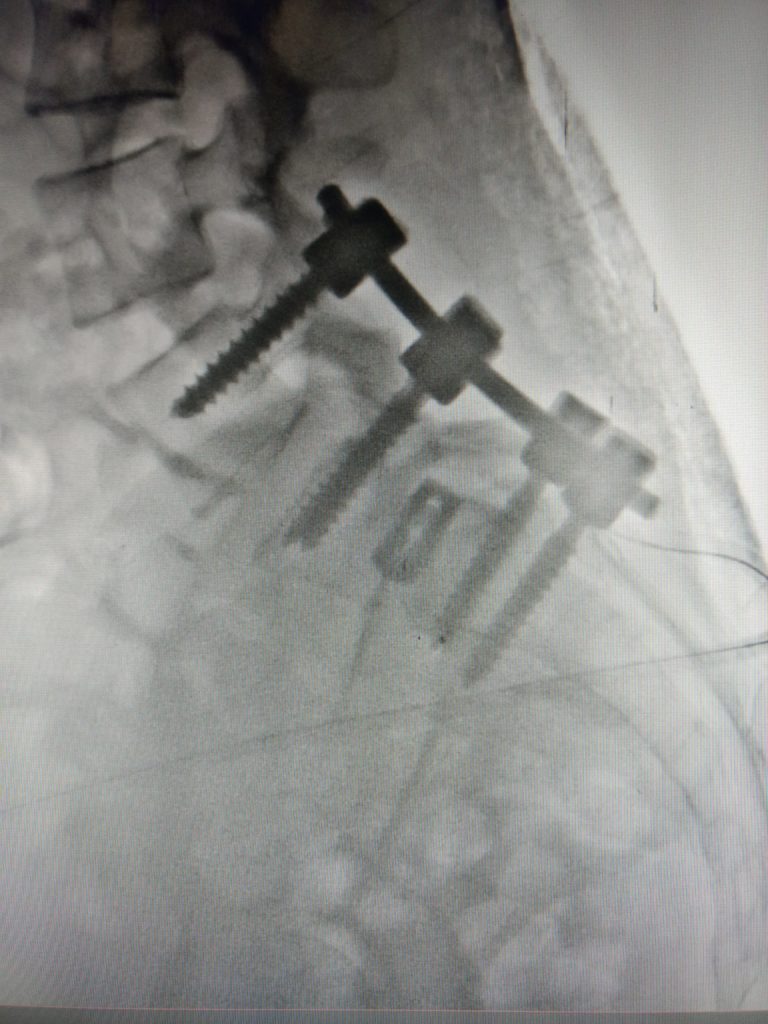
Gr IV anterolisthesis (Spondyloptosis) L5-S1.
Surgery: –
Operated with insitu fixation (cross Delta Fixation) & fusion with fibular bone graft.
Results: –
She started to walk without support from 3rd day of surgery with complete relief in radiating pain. She is working well in farms even hard work after 18 months of surgery.
Patient Speak: –
Highly satisfied.

27 years old guy presented here in post traumatic paraplegia with bladder involvement, after fell down in a well.
Clinical Examinaton: –
No movements at all in both lower limbs, motor power 0/5, AJ & KJ: Absent, Plantar: B/L Mute.
Diagnosis: –
On x ray he had compression wedge fracture with retropulsion , on MRI thecal sac was compressed & intact.
Surgery: –
Decompression with Laminectomy & fixation done immediately with in 24 hrs of injury with scheduled doses of methyl prednisolone.
Results: –
Immediately after surgery there was no improvement but, he started to move his lower limbs from 50 days after surgery & got complete recovery within 7 months of surgery.
Patient Speak: –
Highly satisfied.

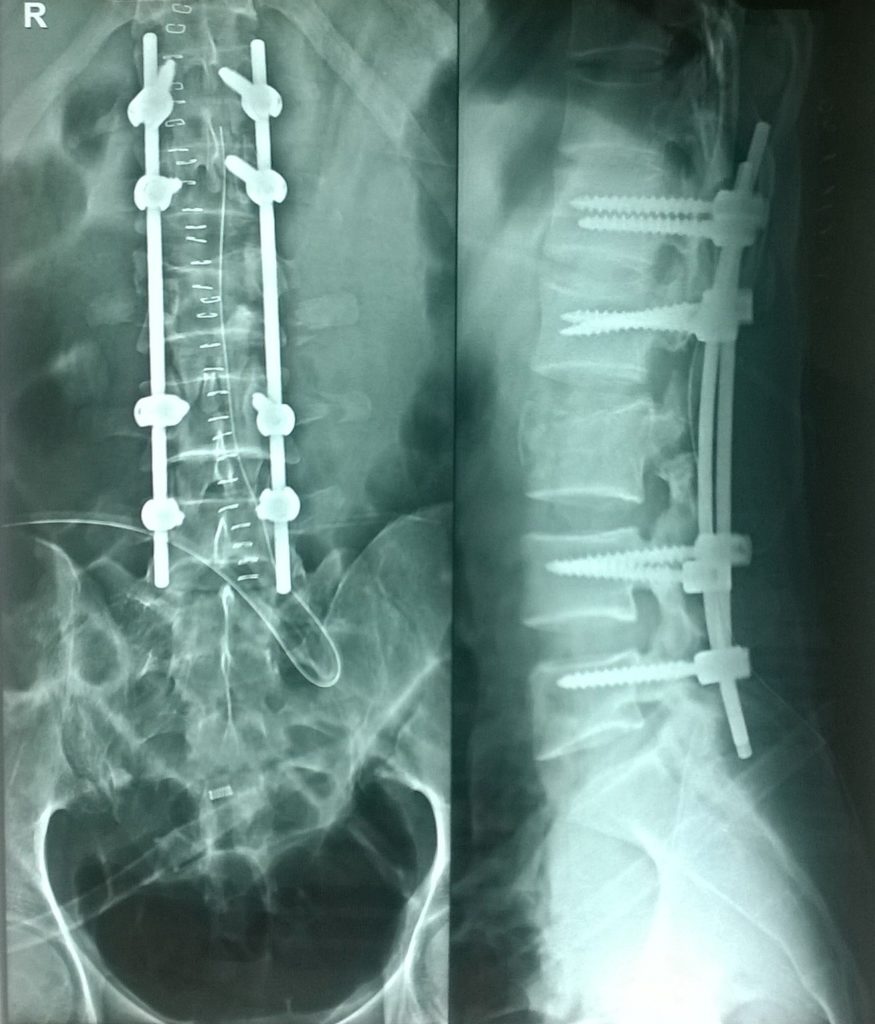
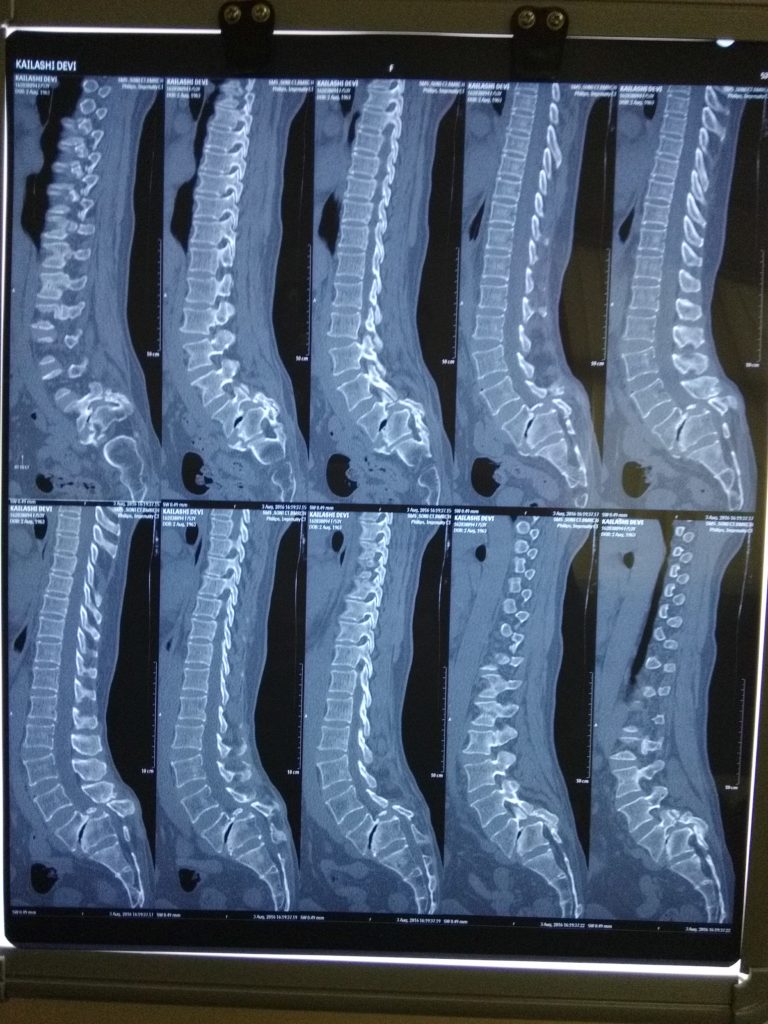
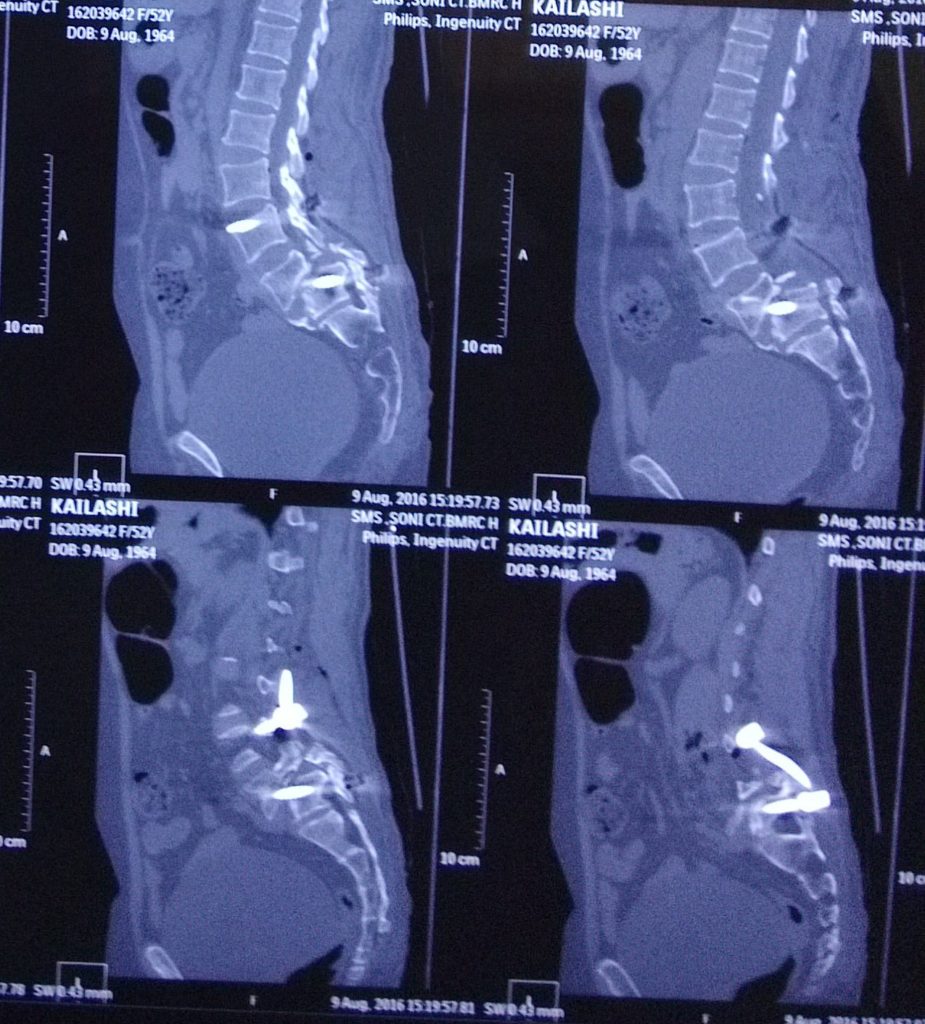
19 years female had LBA radiating to both lower limbs from 5 years, gradually intensity increased, numbness, paraesthesia started in both Lower limbs, when she presented at our clinic she was not able to walk not more than 5 minutes.
Clinical Examinaton: –
Ankle Jerk: Absent (B/L), SLR: Both side 20 degree, Lumbar Lordosis: exaggerated.
Diagnosis: –
After X ray & MRI she diagnosed spodyloptosis (any upper vertebrae lost contact with lower vertebrae & come in front of it).
Surgery: –
Listhesis reduction & TLIF (Translumbar Interbody Fusion with screws, Rods, Cage & Bone Graft).
Results: –
Started to walk from 2nd day of surgery & got Complete relief in radiating pain. On post Operative X ray the listhesis completely reduced.
Patient Speak: –
Highly satisfied.